Staffing relief is hard to come by, call volume is climbing, and patient expectations are rising. A growing number of specialty practices are turning to voice AI to ease the strain – but it’s a crowded market, and it’s hard to tell which vendors actually deliver in live operations. Artera commissioned Signify Research, an independent healthcare research firm, to map how to evaluate voice AI solutions effectively.
Based on primary research with leaders spanning dermatology, ophthalmology, orthopedics and multispecialty groups, this report gives you:
Why specialty leaders still lack a shared definition across the market, the critical difference between inbound and outbound capabilities, and how to sequence adoption to reduce risk.
The demo problem, features vs. workflow depth, integration that’s assumed but never verified, and the change-management and timing gaps that stall otherwise-sound deployments.
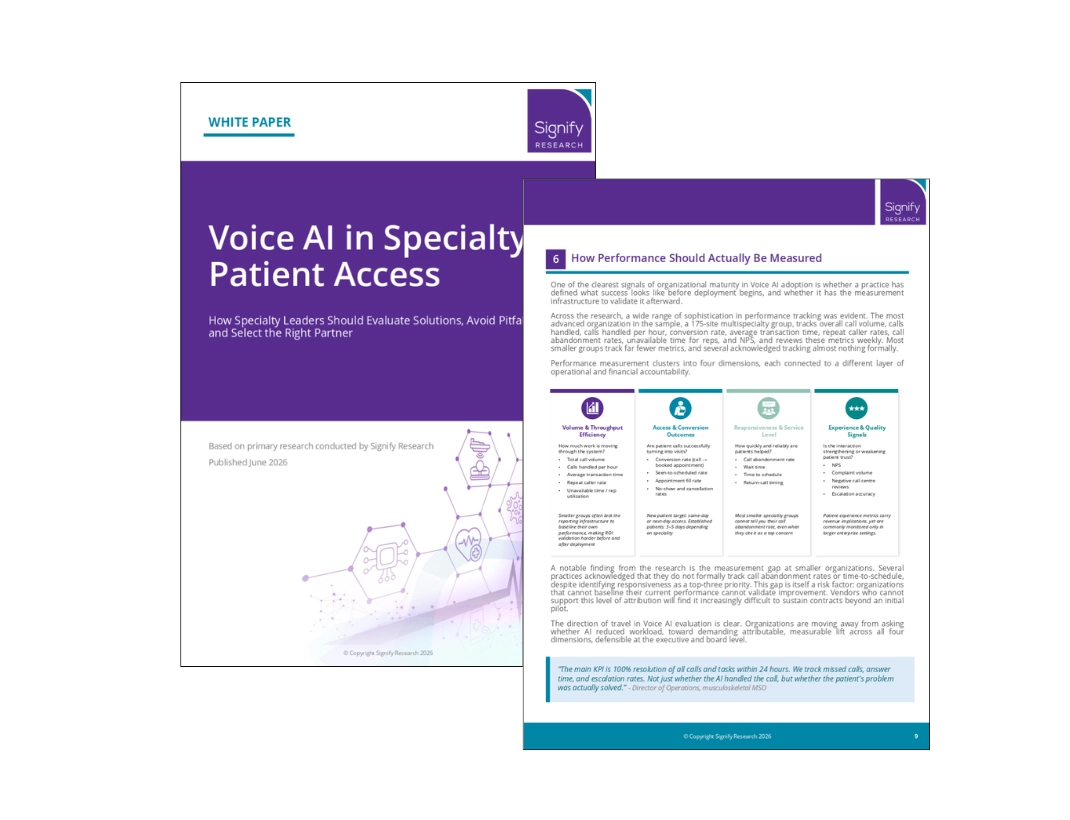
The four dimensions of performance tracking, why a measurement gap is itself a risk factor, and how leading organizations baseline before they buy.
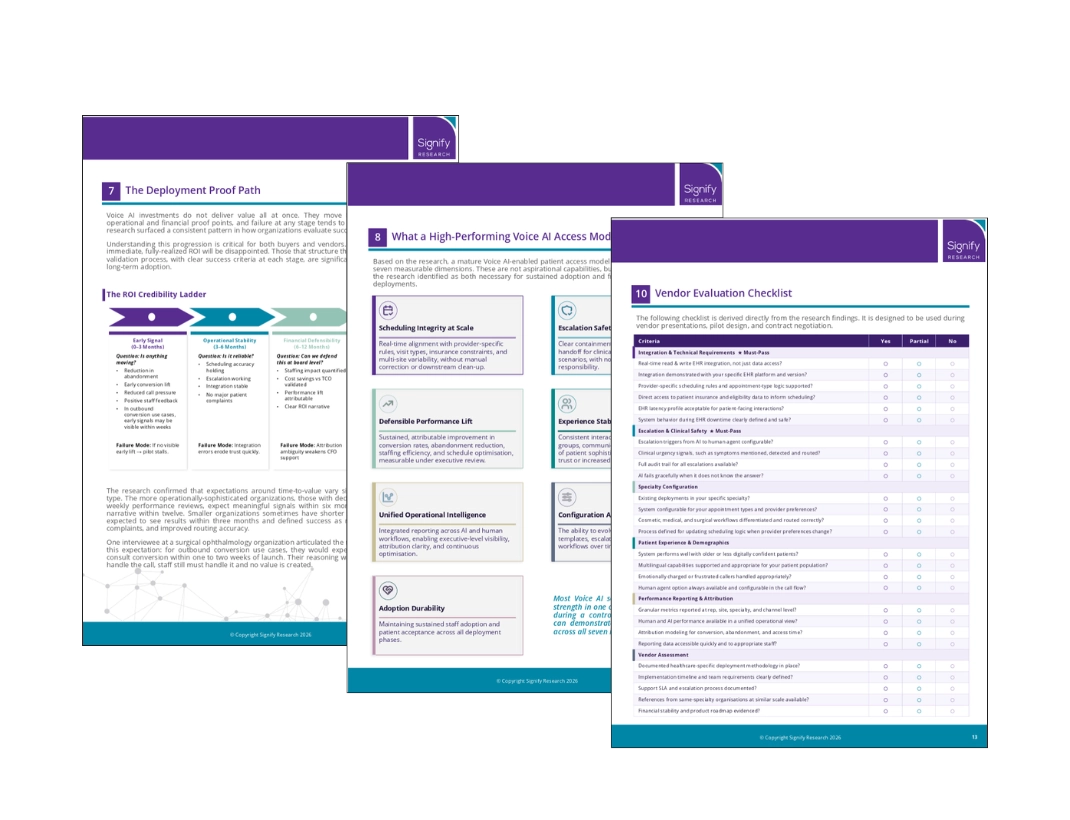
The proof gates every deployment must clear – at 90 days, six months, and twelve – and how to hold a vendor accountable to the same milestones you are.
The five-step approach the most rigorous organizations use to evaluate vendors effectively, including a comprehensive checklist to follow.
Patient access has shifted from an administrative function to a strategic one – tied directly to revenue capture, schedule utilization, and patient retention. That’s exactly why the cost of getting Voice AI evaluation wrong has risen.
There’s a better way to approach it. The organizations that succeed treat adoption as a staged proof process: clear use cases, real-world validation, and vendors held accountable to measurable outcomes at every stage.
The goal isn’t to adopt Voice AI quickly. It’s to adopt it in a way that actually holds up.
A virtual voice agent that handles inbound and outbound patient calls (scheduling, rescheduling, intake triage, basic FAQ, etc.) for specialty groups such as dermatology, ophthalmology, orthopedics, GI, and multispecialty. The agent listens, interprets, replies in natural voice, and writes back into your EHR. The right systems unify scheduling rules, escalation paths, and provider templates inside a single configurable layer.
IVR routes calls through a menu tree and asks the patient to press a digit. Voice AI conducts a conversation, understands intent, accommodates accent and emotion, hands off to a human at the right moment, and writes the completed action back to the EHR in real time. Specialty practices typically layer voice AI onto their existing IVR and telephony stack rather than ripping it out, then progressively shift volume to the AI as it proves out, moving from call routing toward true call resolution.
Force the demo into your real conditions: a multi-provider template, an insurance verification step, a no-show patient asking to be rescheduled three weeks out, a Spanish speaker, a clinical question that must escalate to a human. Then ask the vendor for three references in your specialty at your size, talk to them, and review their post-go-live KPIs. Demos that survive that test are vendors worth a pilot.
Two-way write-back. The voice agent should book, cancel, reschedule, capture demographics, capture insurance, and log the conversation note inside the EHR without manual rework. API access alone is not integration. Ask the vendor to show a live write-back on your test instance, not on their sandbox.
Scheduling integrity, escalation safety, defensible ROI, demographic stability, unified human plus AI intelligence, and configuration agility. The Signify Research report explains each dimension and how leading specialty groups baseline before they buy.
Define success criteria before the pilot. Baseline current call abandonment, schedule fill rate, time-to-third-available-appointment, and front-desk overtime hours. Set proof gates at 90 days, 6 months, and 12 months. Hold the vendor accountable to those numbers, not to demo metrics.
A mismatch between the vendor that won the demo and the operational reality of the practice. Most stalls trace back to thin EHR integration, weak escalation logic, undefined success metrics, and underestimated change-management work, not to the underlying AI model.
Only if escalation logic is explicit and tested. A safe deployment recognizes when a question crosses the clinical boundary and hands the call to a clinician or a triage line without delay. Ask the vendor to walk you through their escalation taxonomy and to demonstrate it live.
Yes. The Signify Research interviews surfaced that many practices cannot baseline current call abandonment, time-to-third-available-appointment, or schedule fill rate. Without those numbers, no vendor can prove lift. Build the baseline first, even if the pilot takes one more month to start.
Artera is the leading provider of agentic patient communications technology for healthcare providers nationwide. Our AI solutions solve front and back-office challenges across the entire patient journey—not just single tasks.
With more than 11 years of experience in patient communications, we're more than a vendor. We're a partner who understands what it takes to navigate operational complexity and deliver real results.
We commissioned this white paper in partnership with Signify Research to give specialty leaders the rigorous evaluation framework this market requires - because choosing the right Voice AI partner shouldn't feel like guesswork.